Streptococcus pneumoniae colonizes the upper respiratory tract of healthy individuals and is one of the most frequent causes of bacterial infection in children. Pediatric infections caused by this pathogen include otitis media (OM), sinusitis, occult bacteremia, pneumonia, meningitis, osteomyelitis, septic arthritis, pericarditis, and peritonitis.
Essential update: New recommendation says high-risk children should receive pneumococcal conjugate vaccine
A new recommendation from the American Association of Pediatrics states that children between the ages of 6 and 18 years with immune deficiency disorders and other high-risk conditions such as HIV, sickle-cell disease, or cerebrospinal fluid leaks should receive a single dose of PCV13. These children should receive the vaccination regardless of prior vaccination status. Also, if these children did not receive PPSV23 previously they should receive a dose of this vaccine no less than 8 weeks after their dose of PCV13. Recommendations for children aged 5 years and younger remain the same.
Signs and symptoms
Children with pneumococcal infections usually have a temperature higher than 102°F, along with symptoms of specific infections, as follows:
- OM – Otalgia, upper respiratory symptoms, vomiting
- Sinusitis – Headache, facial tenderness (much less frequent than in adults), symptoms of upper respiratory tract infection lasting for 10 days or longer
- Occult bacteremia – Fever without a localizing source in children aged 2-24 months
- Pneumonia – Cough; chest pain, shortness of breath, or respiratory difficulty; malaise and poor appetite
- Meningitis – Stiff neck, vomiting, headache (older children); high fever (>103°F), lethargy, irritability, poor feeding, inconsolable crying[2]
Physical findings include the following:
- OM – Bulging, erythematous, or yellow tympanic membrane with poor mobility and purulent fluid seen behind the membrane
- Sinusitis – Tenderness to palpation over maxillary or frontal sinuses, nasal discharge of any color, swollen nasal turbinates
- Bacteremia – None, besides fever (≥102°F) and tachycardia associated with the fever
- Pneumonia – Crackles or decreased breath sounds in the area of lobar consolidation on chest auscultation, with egophony in patients with severe consolidation and dullness to percussion; retractions, tachypnea, or both
- Meningitis or other central nervous system (CNS) infection – Ill appearance; nuchal rigidity (may not be present before age 4 months); altered mental status with poor responsiveness (patient may present in comatose state); other neurologic abnormalities possible (eg, cranial nerve deficits, ataxia, weakness); poor perfusion and signs of shock in patients with concurrent pneumococcal sepsis
Diagnosis
The following laboratory studies are indicated in patients with pneumococcal infections:
- White blood cell (WBC) count and differential
- Antigen tests (cerebrospinal fluid [CSF], urine)
- Gram stain (CSF, synovial fluid, pleural fluid)
- Culture (blood, CSF, pleural fluid, middle ear effusion, synovial fluid)
Specific testing recommendations for particular clinical syndromes are as follows:
- OM or sinusitis – Tympanocentesis and bacterial cultures of middle ear fluid if chronic OM is refractory to antibiotics
- Sinusitis – Culture of sinus fluid if sinusitis is refractory to antibiotics
- Occult bacteremia – Culture of blood (≥2 mL)
- Pneumonia – Blood culture; sputum cultures are difficult to obtain from children, and results may be falsely positive
- Meningitis (suspected) – Lumbar puncture with CSF analysis (cell count, protein levels, glucose levels, Gram stain, culture; antigen tests are needed only in cases of antibiotic pretreatment); blood culture
- Osteomyelitis or septic arthritis – Surgical biopsy or joint aspiration; culture of fluid or bone; blood culture
Imaging studies that may be helpful include the following:
- Chest radiography
- Computed tomography (CT) of the head (often unnecessary)
- Magnetic resonance imaging (MRI) of the head
Management
Antibiotic therapy and supportive care are indicated. The key to successful antibiotic therapy is achieving drug concentrations in the affected area of the body that are several times higher than the minimal inhibitory concentration (MIC) for S pneumoniae.
Recommendations for particular clinical situations include the following:
- OM or sinusitis (initial treatment) – Amoxicillin for 5-10 days (otitis media) or 10-21 days (sinusitis)
- OM or sinusitis that does not improve with standard-dose amoxicillin – High-dose amoxicillin, amoxicillin-clavulanate, cefuroxime, or ceftriaxone (IM)
- Pneumonia (outpatient) – Amoxicillin for 10 days
- Pneumonia (inpatient) – IV ceftriaxone until clinical improvement, then 10 days of outpatient treatment; in critical illness, addition of vancomycin should be considered
- Other invasive pneumococcal diseases – A third- or fourth-generation parenteral cephalosporin (ceftriaxone, cefotaxime, cefepime); in critical illness or the absence of clinical improvement, addition of vancomycin should be considered
- Meningitis – Ceftriaxone or cefotaxime; meropenem may be an alternative in cases of ceftriaxone resistance; vancomycin is always added until susceptibilities are known; rifampin may be added after 24-48 hours of improvement is not noted or the relevant MIC is high
- Penicillin allergy (OM, sinusitis, outpatient treatment of pneumonia) – Azithromycin (or other macrolide), clindamycin, cefuroxime (if there is no cephalosporin allergy), or cefprozil
- Penicillin allergy (inpatient treatment of pneumonia or other invasive infections) – IV ceftriaxone (if there is no cephalosporin allergy); alternatively, IV clindamycin or meropenem; vancomycin may be considered if the patient is severely ill and microbial susceptibility is unknown
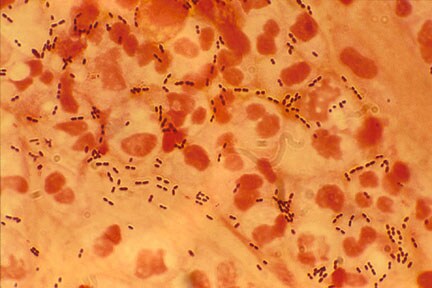
Streptococcus pneumoniae colonizes the upper respiratory tract of healthy individuals and is one of the most frequent causes of bacterial infection in children. Common infections caused by this pathogen include otitis media (OM), sinusitis, occult bacteremia, pneumonia, and meningitis. Pneumococci may also cause osteomyelitis, septic arthritis, pericarditis, and peritonitis. See the image below.

Reference: http://emedicine.medscape.com/article/967694-clinical



1 comment :
I was diagnosed as HEPATITIS B carrier in 2013 with fibrosis of the
liver already present. I started on antiviral medications which
reduced the viral load initially. After a couple of years the virus
became resistant. I started on HEPATITIS B Herbal treatment from
ULTIMATE LIFE CLINIC (www.ultimatelifeclinic.com) in March, 2020. Their
treatment totally reversed the virus. I did another blood test after
the 6 months long treatment and tested negative to the virus. Amazing
treatment! This treatment is a breakthrough for all HBV carriers.
Post a Comment